
Myocarditis in young patient
“A rare presentation of myocarditis in young patient : clinical conundrum. Myocarditis is defined as active inflammatory destruction of the myocardium. A large variety of infectious agents, systemic diseases, drugs, and toxins can cause myocarditis, but...”
October, 2015
M. Glisic, I. Milinkovic, P.M. Stefanovic
 alexraths / 123RF Stock Photo
alexraths / 123RF Stock Photo
Background
Myocarditis is defined as active inflammatory destruction of the myocardium. A large variety of infectious agents, systemic diseases, drugs, and toxins can cause myocarditis, but still the etiology in many particular cases remains undetermined. (1,2) Despite broad array of etiological causes of myocarditis still viral myocarditis remains the prototype, therefore when we consider myocarditis we usually refer to viral myocarditis as its most common form. (3) Epidemiological studies suggest that during the lifetime around 70% individuals in general population will be in contact with cardiotropic viruses, and half of exposed will have an episode of acute viral myocarditis. (4) Recent studies show that most frequent causal agents are Parvovirus B1, Human Herpes Virus 6, Enterovirus (Coxsackie Virus) respectively. (5, 6) Clinical manifestations range from asymptomatic ECG abnormalities with elevated values of cardiac enzymes to fulminant myocarditis presenting as new-onset cardiomyopathy to life-threatening ventricular arrhythmia. Clinical experience showed that most patients remain asymptomatic. (7)
Case presentation
A 20-year-old female was transferred to Department of Heart Failure from Coronary Unit, presenting with acute chest pain, 3 hours after a cocktail consumption (vodka and energy drink).
Medical history: at the age of 15 she was hospitalized at Neurology Department of Institute for Mother and Child Health Care due to ischemic cerebral insult with right-sided hemiplegia, facial nerve paresis and motor aphasia, a week after flulike symptoms with fever. Previously she actively practice athletics and consumed energy boosters (Coenzyme Q10, L- Glutamyl, anabolic minerals, L-Carnitine extreme, Arginine ornithine lysine). A week before CVI occurred she was treated for heavy alcohol intoxication. Echocardiography examination revealed enlarged left ventricle (5.2/4.0cm) with reduced contractility and ejection fraction of around 40%, with three thrombi in apical region of LV. Laboratory showed increase in troponin I, CK –MB and serum transaminases, high antibody titer for Coxackie B4 and increased titer for B. Burgdorferi. She was diagnosed and treated as myocarditis. Blood coagulation tests revealed homozygous C677T mutation for MTHFR gene, which increases risk of thrombosis. Since sinus node dysfunction with extreme bradycardia was detected, she had an ICD implanted.She was discharged with anticolagulant therapy. Neurological deficit completely regressed after rehabilitation. Six months after discharge she had an unsuccessful RF catheter ablation of paroxysmal VT, after which ICD was implanted. In 2012 oral anticolagulant therapy was discontinued due to normal coagulation status, and left ventricular function.
In the mean time she was asymptomatic. Several months before ER admission she had erogospirometry test performed that showed normal functional capacity without evidence of myocardial ischemia. At admission, physical examination revealed a blood pressure of 110/70 mmHg, heart rate of 80 bpm, discreet systolic murmur at the apex, with no evidence of decompensation.
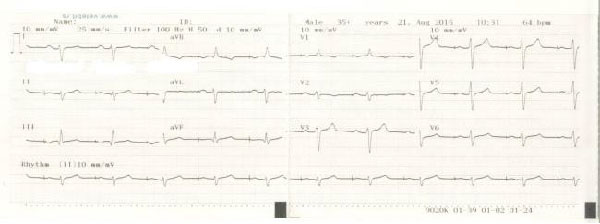
The electrocardiogram revealed sinus rhythm with regular pacemaker pacing, 64 bpm, right heart axis, qR in leads D3 and aVF, negative T wave in lead V1, V2.
Laboratory parameters revealed elevated troponin I (49 ug/L), CK (1193 U/L) and LDH (731 U/L) levels. Inflammatory parameters and D-dimer values were in normal ranges. All tests for standard narcotis were also negative.
Echocardiographic examination demonstrated normal left ventricle diameters (4.9/3.7cm), interventricular septal fibrosis with hypokinesia, ejection fraction around 50%, without intracardial thrombi, and normal right heart parameters.
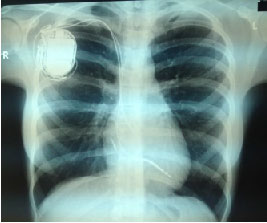
Chest x-ray: without pathological characteristics with visible pacemaker silhouette.
Readings from ICD-DR device showed no significant rhythm and conduction disturbances.
Homocysteine level measured through a routine blood test was 14.9 umol/L wich is considered moderately elevated. Lipoprotein (a) level of 67.3 mg/dl implicates an increased risk for atherosclerosis, heart attack, or stroke. The other parameters (Antithrombin and Protein C) of hemostasis were in normal range.
During hospitalization she was treated with aspirin, low molecular heparin, beta-blockers, mineralocorticoid receptor antagonists and ACE inhibitors. She was discharged 12 days after initial hospitalization, asymptomatic and in stable condition, with beta blocker, Aspirin, folic acid and vitamin B complex therapy and the advice to avoid intensive physical activity.
Discussion
Intracardiac thromosis is rare in younger age. In the last few decades, the incidence of intracardiac thrombosis increased, especially in cases with preexisting hypercoagulable state. (8) The most important predisposing factors for left heart throbosis are dilated cardiomyopathy, atrial fibrillation, endocarditis, prosthetic heart valves, intracardiac tumors and rheumatic mitral stenosis. Left ventricular systolic dysfunction and dilatation are contributing the formation of intracardial trhombi by altering the hemostatic state. Besides that, heart failure is associated with abnormalities of endothelial function, which is also prothrombogenic. In addition, MTHFR gene provides instructions for enzyme methylenetetrahydrofolate reductase synthesis. This enzyme is a part of multistep conversion process of amino acid homocysteine to methionine (conversion of a molecule called 5,10-methylenetetrahydrofolate to a molecule 5-methyltetrahydrofolate). Dysfunction of MTHFR gene leads to elevated homocysteine serum levels (hyperhomocysteinemia). Hyperhomocysteinemia increases risk for atherosclerosis and arterial and venous thrombosis. (9-14). Studies have shown that mean values of homocysteine depend on MTHFR genotype. The most common finding in the general population is mutation of MHTR gene with normal homocysteine and lipoprotein levels. While cases of elevated homocysteine and lipoprotein levels are rare. (19)
In reported case, two of the above mentioned risk factors for intracardial thrombosis were present- left ventricle disfunction caused by myocarditis and predisponing hypercoagulation state. In addition, the risk for instravascular thrombosis was also present, making it plausable as a cause of CVI. Conduction and rhythm disturbances are expected as a complication of myocarditis, and in this patient lead to initial antibradycardial and later, on a permmanent ICD-DR implantation.
Vasospasm can be, also, a possible cause of prolonged ischemia, myocardial infarction or cerebrovascular insult. Reversible cerebral vasoconstriction syndrome (RCVS) is characterized by reversible narrowing of the cerebral arteries. It is usually associated with use of vasoactive agents (drugs that modulate dopamine or serotonin system or sympathomimetics), but can be idiopathic, as well. The most common symptoms are acute headache followed with neurologic deficit. (15) Energy drinks are one of most commonly used substances which have sympathomimetic effects Thier main compound –cafeine is an antagonist of adenosine and presynaptic α1 receptor and it causes the increase in catecholamine release and vasoactive effects. (16) Energy drinks usually contain additional herbal ingredients (ginkgo biloba leaf extract, Siberian ginseng root extract,) with significant sympathomimetic properties. Worrall et al published a report of cerebral vasculopathy and stroke after single consumption of an herbal energy drink. (17,18) Wilson et al. presented a case of 17-year-old male who had been diagnosed with transient coronary vasospasms as a result of drinking a disproportionate amount of caffeinated energy drinks.
During second hospitalization for suspected myocarditis, the acute coronary syndrome was also taken into consideration as a cause of chest pain and elevation of cardiac specific enzymes. Coronary angiography wasnt perfomed due to atypical clinical presentation, absent ECG signs of ischemia, normal echocardiographic findings and patient’s age.
Patient was discharged with folic acid and B- vitamin complex therapy of elevated homocysteine and lipoproteine a levels and Aspirin was adviced as permament treatment. Since she has history of energy boosters and alcohol consumption before both hospitalizations of interest, she was adviced to avoid energy drinks consumption in the future.
With respect to mentioned findings there were not enough criteria for myocarditis nor enough sings of acute myocardial ischemia. It remains unclear whether thromboembolic CVI at age of 15 was a direct consequence of myocarditis and embolisation from LV trombi precipitated by reduced LV function and coagulation disorder. It is also uncertain, wheater a nonspecific chest pain at the age of 20 was caused by energy booster-induced vasoconstriction, premature atherosclerotic disease in the coronary arteries, or was it a combination of all these factors.
References
- Richardson et al. Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of cardiomyopathies.Circulation1996;93:841–842.
- Leone O et al. 2011 Consensus statement on endomyocardial biopsy from the Association for European Cardiovascular Pathology and the Society for Cardiovascu- lar Pathology. Cardiovasc Pathol 2012;21:245–274.
- Baboonian C, Treasure T. Meta-analysis of the association of entero- viruses with human heart disease. Heart. 1997;78:539 –543.
- O’Connell JB: The role of myocarditis in end-stage dilated cardiomy- opathy. Tex Heart Inst J 1987, 14:268–275
- Kuhl U, Pauschinger M, Noutsias M, et al. High prevalence of viral genomes and multiple viral infections in the myocardium of adults with “idiopathic” left ventricular dysfunction. Circulation 2005;111:887-93
- Caforio AL1 at al. European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: aposition statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases.Eur Heart J. 2013 Sep;34(33):2636-48, 2648a-2648d. doi: 10.1093/eurheartj/eht210. Epub 2013 Jul 3
- Dec GW. Introduction to clinical myocarditis. In: Cooper LT, ed. Myocarditis: From Bench to Bedside. Totowa, NJ: Humana Press; 2003: 257–281. However when the disease has more severe form we should be aware of possible complications and try to prevent them.
- Atalay S, Akar N, Tutar HE, Yilmaz E. Factor V 1691 G-A mutation in children with intracardiac thrombosis: a prospective study. Acta Pa-ediatr 2002;91:168-71.
- Kádár K, Hartyánszky I, Király L, Bendig L. Right heart thrombus in infants and children. Pediatr Cardiol 1991;12:24-7.
- Ross P Jr , Ehrenkranz R, Kleinman CS, Seashore JH. Thrombus associated with central venous catheters in infants and children. J Pediatr Surg 1989;24:253-6
- Tegeler CH, Downes TR. Thrombosis and the heart. Semin Neurol 1991;11:339-52.
- Lip GY, Gibbs CR. Does heart failure confer a hypercoagulable st-ate? Virchow’s triade revisited. J Am Coll Cardiol 1999;33:1424-6. 7) Meltzer RS, Visser CA, Fuster V. Intracardiac thrombi and systemic embolization. Ann Intern Med 1986;104:689-98.
- Treasure CB, Vita JA, Cox DA, et al. Endothelium-dependent dilation of coronary microvasculature is impaired in dilated cardiomyopathy. Circulation 1990;81:772-9.
- Varga EA1, Sturm AC, Misita CP, Moll S. Cardiology patient pages. Homocysteine and MTHFR mutations: relation to thrombosis and coronary artery disease. Circulation. 2005 May 17;111(19):e289-93.
- Chen SP, Fuh JL, Wang SJ. Reversible cerebral vasoconstriction syndrome: current and future perspectives. Expert Rev Neurother. 2011;11:1265-1276.
- Benowitz NL. Clinical pharmacology of caffeine. Annu Rev Med. 1990;41:277-288.
- Wilson, R. E., Kado, H. S., Samson, R., & Miller, A. B. (2012). A case of caffeine-induced coronary artery vasospasm of a 17-year old male. Cardiovascular Toxicology. doi:10.1007/s12012-011- 9152-9.
- Debopam S. Reversible cerebral vasoconstriction syndrome: another health hazard of energy drinks? Clin Pediatr (Phila). 2015 Feb;54(2):186-7. doi: 10.1177/0009922814541675. Epub 2014 Jul 7
- Intessar ES, Effect of Methylenetetrahydrofolate Reductase Gene Mutation on Plasma Homocysteine Level and its Prevalence in Arterial Diseases. J. Taibah Uni. Med. Sci. Volume 1, Issue 1, 2006, Pages 20–29
Poster presentation, International congress Neurocard, Belgrade 2015